
Greetings. I just wanted to relay some observations of how we have improved care in the Intensive Care Unit at the hospital I am at. There are simple interventions you can implement in your own space or institution that will improve quality of care, communication, team dynamics, and patient safety. The unit is a very dynamic place and requires closer monitoring and attention.
In the Unit we have instituted afternoon rounds and midnight rounds where the resident and on-call intern will review the plan for the day and figure out which items have been completed. We will then evaluate the patient via vitals/physical exam/nurse input and discuss the plan for the late afternoon/evening. We then will create an assessment/plan for the next eight hours. During this time we also review medications and discontinue those that are no longer needed or require dose adjustment.
Another intervention is the creation of ventilator bundle set and sepsis bundle sets that are a checklist protocol based system that can be applied to a patient in situations where they need to intubated or taken care of when in sepsis. This allows us to make sure we have incorporated evidence based strategies in taking care of patients that require activation of these bundles.
We also are in the midst of creating Tuesday School (A 4 hour long protected time where residents/medical students participate in interactive medical education with application of numerous topics such as quality improvement and patient safety.
It would be fantastic to create opportunities for medical students in their curriculum during 3rd year with each rotation to spend 1 hour during the month learning basics of quality improvement. The idea would be to engage them to start thinking an observing in a way that may lead to ideas for interventions resulting in quality improvement.
I would be interested in hearing about other interventions and ideas folks have.
For those folks in Boston please make sure you attend the event on 4/23 at Harvard Medical School from 6:30 pm - 9:00 pm where we will go through a case discussion and network with other like minded faculty and students.
Also, Dr. David Nash from Jefferson Medical College will be discussing how to get quality improvement into your curriculum on 4/27 from 4:30-5:30 EST. It will also be a time for you to ask questions and learn some concrete skills.
Have a great weekend!
Jay
Apr 16, 2009
IHI Open School Boston Regional Event NEXT Thursday!
If you are in the Boston area...Mark Your Calendars!
Several Boston Chapter Leaders have collaborated to host an IHI Open School Boston Regional Event on Thursday, April 23rd from 6:30-9:00p.m. at the Harvard Medical School.
Registration is free and food and beverages will be provided. We now have 8 Chapters in the Boston area and I know they’d love to meet with local QI leaders and students. All students, faculty, and health professionals are invited to attend. Please share this with others. If you would like to attend any part of the event, please register by following this link.
I hope to see you all there!
Several Boston Chapter Leaders have collaborated to host an IHI Open School Boston Regional Event on Thursday, April 23rd from 6:30-9:00p.m. at the Harvard Medical School.
6:30-7:00 – Introduction/Ice Breaker
7:00- 8:00 – Case Study Discussion facilitated by Dan Hunt, MD and Meridale Vaught, MD from MGH
8:00-9:00 – Social/Networking
Registration is free and food and beverages will be provided. We now have 8 Chapters in the Boston area and I know they’d love to meet with local QI leaders and students. All students, faculty, and health professionals are invited to attend. Please share this with others. If you would like to attend any part of the event, please register by following this link.
I hope to see you all there!
Apr 15, 2009
Getting Quality Improvement into the Curriculum: On Call with Dr. David Nash

Interested in having quality improvement and patient safety in the curriculum at your school? Wish you knew how you could help make it happen?
Join us for an On Call Event with David Nash
Monday, April 27, 2009 – 4:30-5:30 pm Eastern
David B. Nash, MD, MBA. Dr. Nash is the founding dean of the Thomas Jefferson University Jefferson School of Population Health, which just launched a new master's degree in Healthcare Quality and Safety.
You'll learn:
- What it took to create Jefferson's new Healthcare Quality and Safety master's degree
- How to effectively make the case to faculty or administrators for inserting quality and safety into your curriculum - and what you can realistically expect as a response
- How you can get the quality and safety skills you need now when there isn't a formal way to do so at your school
Join this free call! Advance registration is required. Click here to register!
Follow this link to download materials for the call.
This free call is part of a monthly audio conference series that brings experts in health care improvement together with students from medicine, nursing, dentistry, pharmacy, health care management, public health, and other allied health professions. Each hour-long call is moderated by a student, ends with a question-and-answer period, and focuses on an issue that affects you. Visit our website to download audio files or written transcripts of past On Call audio conferences.
Hope to see you all on the call!
Apr 13, 2009
A Big Step Foward in the Health IT Race
The spread of new ideas and technology are interesting phenomena to observe and study. In the social networking world, Friendster led to Facebook and MySpace and where does Twitter fit in? When it comes to adopting new technology, those under the age of 25 tend to adopt things faster than those over the age of 65. Or to put it this way, it's not uncommon for me to see a group of middle school students jamming to their iPods while texting on their cell phones. But, watching a video of my 94 year-old grandmother playing Wii Bowling rocked my world!
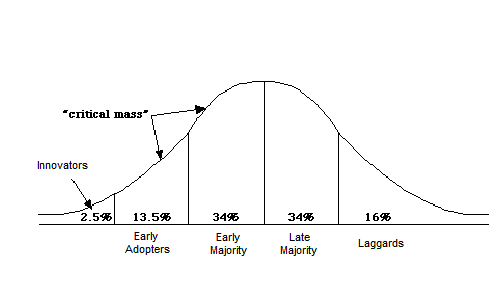
In a book titled Diffusion of Innovations written by Everett Rogers, Rogers outlines a model for the adoption and diffusion of innovation. When it comes to adopting new technology, health care is notoriously known to be part of the "late majority" or "laggard" groups. Some argue that the use of internet computing for communication in health care has not changed in decades!
Well, that is all hopefully beginning to change. The recently enacted stimulus bill — the American Recovery and Reinvestment Act of 2009 (ARRA) has allocated $19 billion to promote the adoption and use of health information technology (HIT), with a focus on electronic health records (EHRs). In a Perspectives piece published in the New England Journal of Medicine on April 9th, Dr. David Blumenthal, the newly appointed National Coordinator for Health Information Technology, discusses the challenges and goals of stimulating the adoption of HIT.
As discussed in the piece, currently, only 17% of US doctors and only 10% of US hospitals are using even the most basic form of EHR. Because of the substantial upfront cost, the perceived lack of financial return from investing in HIT, the technical and logistical challenges involved in installing, maintaining, and updating them, and consumers' and physicians' concerns about the privacy and security of electronic health information, the medical field has decided not to jump on the technology bandwagon. While Washington DC does have a plan to incentivize physicians and health systems to adopt EHR through Medicare and Medicaid benefits, much work needs to be done. Substantial investments need to be made to create an interoperable system that is flexible to new technology updates, yet provides security and privacy. President Obama has promised that by 2014 every American will benefit from having a personal EHR. Just like the IHI WHO Surgical Safety Checklist Sprint, laying down the foundations of this HIT system will be a race--not quite a marathon in duration. Let's call it the 10K HIT race.
Since the HIT race started with announcement of the ARRA, President Obama and several partnerships have provided several refreshing swigs of water. Last Thursday, President Obana, along with Department of Defense (DoD) Secretary Robert Gates and Veterans Administration (VA) Secretary Eric Shinsheki, announced the commitment to create a Joint Virtual Lifetime Electronic Record, a system to computerize medical records for all military personnel. This Joint Virtual Lifetime Electronic Record would effectively bridge the records the DoD holds on active-duty men and women and the records the VA holds on veterans. With the military leading the way as it has done on several occasions in the past, President Obama is sending the message that an investment in HIT is not just to bring technology to health care, but to improve the quality of health care delivery, the health of populations, and the efficiency of our health systems. President Obama hopes that the military system will become a model for the rest of the nation to adopt. Click here to read the release.
Side note: Dr. Don Berwick was asked to appear on NewsHour with Jim Lehrer to discuss this new announcement of a streamlined military EHR and its implications on health care. See the video below!
Having trouble viewing? Click here to watch a streaming video clip, read the transcript, or download the audio clip.
Other spurts of refreshing water have come from partnerships. GE Healthcare announced a partnership with both the CDC and Johns Hopkins to create an easy way to report and target alerts on epidemics. Click here to read Business Week's coverage. Mayo Clinic has partnered with IBM to create a website to consolidate the tools used to search records and data of all kinds. Click here to read The New York Times' report on the new project called, the Open Health Natural Language Processing Consortium.
What other sorts of sprints or 10K races has the government or military led in the past? What features of an EHR are most important to you? How do you think EHRs will transform health care delivery?
In a book titled Diffusion of Innovations written by Everett Rogers, Rogers outlines a model for the adoption and diffusion of innovation. When it comes to adopting new technology, health care is notoriously known to be part of the "late majority" or "laggard" groups. Some argue that the use of internet computing for communication in health care has not changed in decades!
Well, that is all hopefully beginning to change. The recently enacted stimulus bill — the American Recovery and Reinvestment Act of 2009 (ARRA) has allocated $19 billion to promote the adoption and use of health information technology (HIT), with a focus on electronic health records (EHRs). In a Perspectives piece published in the New England Journal of Medicine on April 9th, Dr. David Blumenthal, the newly appointed National Coordinator for Health Information Technology, discusses the challenges and goals of stimulating the adoption of HIT.
As discussed in the piece, currently, only 17% of US doctors and only 10% of US hospitals are using even the most basic form of EHR. Because of the substantial upfront cost, the perceived lack of financial return from investing in HIT, the technical and logistical challenges involved in installing, maintaining, and updating them, and consumers' and physicians' concerns about the privacy and security of electronic health information, the medical field has decided not to jump on the technology bandwagon. While Washington DC does have a plan to incentivize physicians and health systems to adopt EHR through Medicare and Medicaid benefits, much work needs to be done. Substantial investments need to be made to create an interoperable system that is flexible to new technology updates, yet provides security and privacy. President Obama has promised that by 2014 every American will benefit from having a personal EHR. Just like the IHI WHO Surgical Safety Checklist Sprint, laying down the foundations of this HIT system will be a race--not quite a marathon in duration. Let's call it the 10K HIT race.
Since the HIT race started with announcement of the ARRA, President Obama and several partnerships have provided several refreshing swigs of water. Last Thursday, President Obana, along with Department of Defense (DoD) Secretary Robert Gates and Veterans Administration (VA) Secretary Eric Shinsheki, announced the commitment to create a Joint Virtual Lifetime Electronic Record, a system to computerize medical records for all military personnel. This Joint Virtual Lifetime Electronic Record would effectively bridge the records the DoD holds on active-duty men and women and the records the VA holds on veterans. With the military leading the way as it has done on several occasions in the past, President Obama is sending the message that an investment in HIT is not just to bring technology to health care, but to improve the quality of health care delivery, the health of populations, and the efficiency of our health systems. President Obama hopes that the military system will become a model for the rest of the nation to adopt. Click here to read the release.
Side note: Dr. Don Berwick was asked to appear on NewsHour with Jim Lehrer to discuss this new announcement of a streamlined military EHR and its implications on health care. See the video below!
Having trouble viewing? Click here to watch a streaming video clip, read the transcript, or download the audio clip.
Other spurts of refreshing water have come from partnerships. GE Healthcare announced a partnership with both the CDC and Johns Hopkins to create an easy way to report and target alerts on epidemics. Click here to read Business Week's coverage. Mayo Clinic has partnered with IBM to create a website to consolidate the tools used to search records and data of all kinds. Click here to read The New York Times' report on the new project called, the Open Health Natural Language Processing Consortium.
What other sorts of sprints or 10K races has the government or military led in the past? What features of an EHR are most important to you? How do you think EHRs will transform health care delivery?
Apr 11, 2009
"Mistaken Identity"
Here's a great poem from Pulse Magazine.


"Mistaken Identity"
by Kathleen Grieger
Surgery finished,
I finally sleep
Pushing my shoulders,
the technician wakes me
"Come now,
we need a chest x-ray"
Smiling, she pulls me
into position
The x-ray machine
tight against me
Finally getting a chance,
I ask what she is doing
"Oh," she says "I have
the wrong one
You are not a 64
year old male"
Lying me down,
she walks away
As I fall back to sleep,
I wonder, now bald
what I must
look like

About the poem: "Frustrated with the problems and errors that were hugely complicating my medical treatment after brain surgery, I realized that it was necessary for me to start writing again. Because I'd been so busy before, my poetry had been set aside; picking it up again was the best thing I've ever done."

Questions/Comment:
1. As a health care provider, do you use a creative outlet to express your stress or frustration with work? What do you do?
2. What steps are you taught to make sure you have the right patient? Does anyone teach you this? Or, what steps does your health care organization take to make sure you operate on the correct patient?
3. Have you ever had an experience like the patient in the poem?
Introduction to Myself!
Hi, everyone! I was very excited to be invited to write for this blog. As a soon-to-be intern, I enjoy the opportunity to document my experiences both in the field of family medicine and quality improvement. My hope is to use this blog to not only document what I am seeing and doing, but also to use it as an opportunity to reflect upon and discuss issues related to the larger issues of healthcare quality and patient safety. I am also excited to depict how these issues will flavor my experiences as a resident. Lastly, I agreed to write for this blog because that act of writing, itself, relaxes me.
Before I get into any discussion of my experiences in QI or as Aultman Hospital’s Open School President, I feel that I should tell you more about myself. I would like to do this, because the descriptions of my experiences may be skewed by my beliefs, experiences, etc. How am I different than you? How am I the same as you? I would like you to know these things and analyze my writings in light of this information.
I am an only-child. Both of my parents are from the Philippines. Neither of my them are physicians. My mother is a nurse, and my father is a retired engineer. He has diabetes and has had multiple complications related to the disease. I am Catholic. I was born and raised in Cleveland, Ohio. I have attended a private Catholic grade school, and a private Jesuit high school. I did my undergraduate learning at St. Louis University. I briefly considered training to get a Ph. D. in psychology during college. Therefore, I did one year of research at Washington University of St. Louis in the hopes that such an experience would help me make up my mind. I decided that bench research took me too far away from the sort of ‘helping’ that I had always envisioned myself doing. So, I took the MCAT and came back to Ohio to attend medical school. There, I found my passion and niche in primary care.
My interest in QI and PS stems from multiple experiences in the realm of medicine. I remember how frustrated I felt when I learned (on more than one occasion) of the mistakes that hospital staff made while my father was under their care. I remember my mother’s stories of her being witness to less than optimal quality care by some of the hospital staff. As a medical student, the gap that lies between what one learns in the classroom and what one actually experiences on the wards is, at first, shocking.
I knew that I wanted to make a difference in this aspect of medicine.
Today, I am currently the Founder/President of the IHI Open School at Aultman Hospital, which is a community hospital in Canton, Ohio. I am a 4th year medical student at the Northeastern Ohio Universities College of Medicine in Rootstown, Ohio. I will be doing my residency in family medicine at the Mayo Clinic in Jacksonville, FL.
My current favorite band is Coldplay. I relax by going to the gym, writing, and cooking. I am a fan of the Cleveland Cavaliers.
So, that’s me. My next post will be about the starting of a hospital-based Open School Chapter – what worked, what did not. If you have anything else that you would like to know or any topics that you would like me to cover in this blog now or in the future, please let me know.
Again, I am excited to be able to share my experiences and thoughts with you all!
Apr 9, 2009
Timeout? No thanks. With stakes this high, I’d rather keep working.
 As a medical student who is both only weeks away from graduation (Duke, please don’t withhold my diploma) and a long-time admirer of Dr. Groopman’s work, it is with some trepidation that I respond to the recent opinion piece in the Wall Street Journal “Why ‘Quality’ Care Is Dangerous” by Jerome Groopman and Pamela Hartzband.
As a medical student who is both only weeks away from graduation (Duke, please don’t withhold my diploma) and a long-time admirer of Dr. Groopman’s work, it is with some trepidation that I respond to the recent opinion piece in the Wall Street Journal “Why ‘Quality’ Care Is Dangerous” by Jerome Groopman and Pamela Hartzband.However, the issue of healthcare quality improvement is too important for me to ignore such a potentially damaging editorial. Strangely, the article reminded me of a variety of clichés often used to argue against well-intentioned words of caution (such as those of Groopman and Hartzband) including, “Don’t throw the baby out with the bathwater;” “Don’t let the perfect be the enemy of the good,” and “Rome wasn’t built in a day.”
These clichés aren’t excuses. Progress has got to start somewhere, and while we have a long way to go, patients are far better off today than they were in November of 1999 thanks to the myriad efforts of so many dedicated quality improvement champions. Unfortunately, Groopman and Hartzband give only a brief nod to this progress.
 By largely ignoring the successes and claiming that early missteps in particular quality efforts (namely public reporting and pay-for-performance) are examples of the system gone awry, the authors are doing patients and medical progress a serious disservice. They call for a “time out” in the progression of our healthcare system towards increased accountability and improved quality. (And let’s ignore for a moment the potential harm caused by the title of the article which implies that the entire spectrum of quality improvement efforts is dangerous).
By largely ignoring the successes and claiming that early missteps in particular quality efforts (namely public reporting and pay-for-performance) are examples of the system gone awry, the authors are doing patients and medical progress a serious disservice. They call for a “time out” in the progression of our healthcare system towards increased accountability and improved quality. (And let’s ignore for a moment the potential harm caused by the title of the article which implies that the entire spectrum of quality improvement efforts is dangerous).Are there problems? Yes. Are there inherent risks in any major changes to a system as complex as the U.S. healthcare system? Of course. In fact, the article articulates many of the risks and, to date, failures of some of these efforts (which I hope to discuss in more detail in a follow-up posting). However, those of us who are patients, have friends or family who are patients, take care of patients, or simply pay taxes, should not accept the “time out” called for by Groopman and Hartzband; especially since I don’t remember seeing any breaks or timeouts in continuous quality improvement cycles.

Subscribe to:
Posts (Atom)


{kind=link}
{kind=link}